
Consider these staggering stats that capture the worldwide prediabetes and diabetes epidemic:
Worldwide:1
- 463 million adults (aged 20-79) have diabetes (6% of world population)
- By 2045 the diabetes population is estimated to reach 70 million
- 1 in 5 people aged 65 or older have diabetes
- 1 in 2 people (232 million) have diabetes but remain undiagnosed
- 374 million people are at increased risk of developing type 2 diabetes (5% of world population)
- $760 billion dollars were spent to provide care for people with diabetes in 2019
United States:
- 34.2 million people have diabetes (10.5% of U.S. population)2
- By 2060 the diabetes population is estimated to reach 61 million (18% of U.S. population)3
- 95% of people have type 2 diabetes whereas 5% (1.6 million) have type 1 diabetes.2 Though type 1 diabetes is thought of as a young person’s disease, about 1 million adults (20 years and older) have it4
- 7.3 million adults (aged 18 years and older) (2.8%) have diabetes but remain undiagnosed
- 27% of adults aged 65 years and older have diabetes
- 88 million adults (aged 18 years and older) (26%) are estimated to have prediabetes*
- $327 billion dollars were spent on direct and indirect for people with diabetes in 20175
Global Call to Action to Prevent or Delay Prediabetes and Type 2 Diabetes Progression
Without a doubt, overweight and obesity track closely with the onset and diagnosis of prediabetes. Nearly 90% of U.S. adults 18 years and older with diabetes (type 1 and 2) are overweight or have obesity.2 A multitude of factors promote rising rates of overweight and obesity including excess calories, inadequate physical activity, sedentary lifestyles, and the list goes on...
Here’s the pressing question: As the pandemics of prediabetes and type 2 diabetes fast approaches what actions can people and populations take to prevent or delay these conditions? For starters, don’t think of them as two diseases. Prediabetes and type 2 diabetes are a continuum that may be kicked into gear due to genetics (family history) and further exacerbated by excess weight. This situation typically triggers a cascade of effects that results in insulin resistance (the body’s inability to use the insulin it produces), and in response overproduction of insulin. That is until the body can no longer produce sufficient insulin to keep glucose levels in a normal range. It’s at this juncture that prediabetes progresses to type 2 diabetes.
Global Studies Underscore Importance of Early Action, Healthy Weight and Glucose Control
Need positive news? Here it is!
About prediabetes: Long term studies conducted around the globe from China to Finland and the U.S., over the last 30 plus years, focused on whether type 2 diabetes could be prevented or delayed in people at high risk or with prediabetes.6 While the studies differed slightly in their designs, all had as their foci lifestyle changes, including actions to make healthier food choices, improve eating habits and become more physically active with the end goal to promote weight loss and keeping lost pounds off. In sum these studies showed that losing at least 5% of body weight, even with some weight regain over time, can prevent or delay progression of prediabetes to type 2 diabetes.
About type 2 diabetes: Two large studies were conducted among people in their early years with type 2 diabetes. The one conducted in the U.S. is Look AHEAD7 and the study conducted in the United Kingdom is DiRECT UK.8 The bottom lines? Both studies showed that with weight loss (at least 5-7%), and keeping off as many of those lost pounds as possible overtime, people either prevented or slowed their progression of type 2 diabetes. Some even put type 2 diabetes into remission.8 Of note, losing 5% of weight or more has been shown to significantly improve A1C (average glucose levels), blood lipids and blood pressure and more. For some people these benefits often occurred with the use of less and/or fewer medications to manage one or more of these conditions.7-9 More weight loss (7% or more) produces an even longer list of clinical, physiological and psychological benefits.7-10
What to Eat with Prediabetes and Type 2 Diabetes
The American Diabetes Association in 2019 published their update on nutrition guidance - Nutrition Therapy Consensus Report For Adults With Diabetes and Prediabetes.10 The report underscores four key messages that I collectively refer to as, “eating pattern common denominators”:
- Emphasize consumption of non-starchy vegetables;
- Minimize consumption of added sugars and refined grains;
- Choose whole foods over highly processed foods; and
- Replace sugar-sweetened beverages with water as often as possible.
These “eating pattern common denominators” focus squarely on actions to take when choosing carbohydrate-containing foods. This guidance concludes that reducing (not severely restricting or eliminating!) the total amount of carbohydrate one eats has the most support for improving glucose levels long term.10 A second focus is on quality. Choose sources of carbohydrate that contain one or more of the following: whole grains, dietary fibers, and vitamins and minerals. Keep sources of carbohydrate that contain added sugars, unhealthy fats and sodium, to a bare minimum.
But there’s now a new twist to the discussion about high quality sources of carbohydrate to mention. That is a well-researched food and beverage ingredient, called PalatinoseTM (brand name for isomaltulose). Research shows that by regular consumption of a sufficient amount of this slow-release source of high quality carbohydrate, can reduce the rise of blood glucose after eating more so than some sources of healthy carbohydrate.11-17
More about Palatinose™ – A Slow Release Carbohydrate
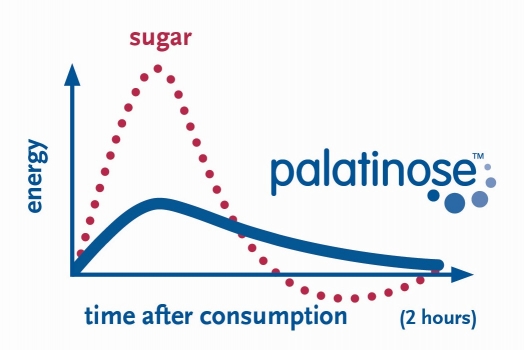
Research on the ingredient isomaltulose, conducted over the last few decades, shows that it releases its energy (calories) more slowly than other carbohydrate-containing ingredients.12 For people with prediabetes and type 2 diabetes, the slower release of energy can offer two benefits. One is to provide a more sustained supply of energy over the next few hours after consuming a product with the ingredient.12-14 Two is a slower and overall lower rise in blood glucose after consuming the food. Research shows that these two benefits result in less insulin (made by the pancreas) being needed and released.14,15,17
The cascade of events that occur after consuming Palatinose™ results in a healthier response from several gut hormones, known as incretins.11,17 It produces a lower release of the hormone, Gastric Inhibitory Peptide (GIP) in the upper part of the small intestine and a larger release of Glucagon-like Peptide-1 (GLP-1) in the lower part of the small intestine. Add to these benefits Palatinose™ also burns more energy (calories) from fat, when being metabolized.13 This benefit has been linked to a small amount of weight loss when it is replaced for sugar (sucrose) in an eating plan.
As an ingredient for food and beverage manufacturers, Palatinose™ is made from naturally occurring sugar beet18 Manufacturers are using Palatinose™ in an increasing number of foods and beverages as a naturally sourced high quality carbohydrate ingredient. It is typically used in place of ingredients like maltodextrins or traditionally-used sugars that raise glucose more quickly, to take advantage of Palatinose’s™ slow glucose release properties. Replacing foods that use the ingredient Palatinose™ for those that contain high quality carbohydrate but are quickly absorbed may help people with prediabetes and diabetes reduce glucose fluctuations and decrease insulin needs over the course of the day.11-17 To find products with Palatinose™ search on the term ‘isomaltulose’ and look for ‘isomaltulose’ on product ingredient labels. Taking this action is certainly worth a try!
Learn more about Palatinose™and review the extensive reference list.
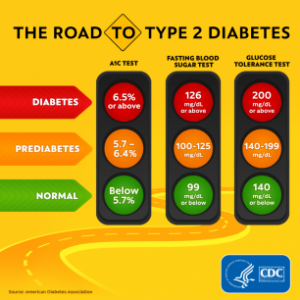
*Prediabetes is defined as fasting plasma glucose values of 100 to 125 mg/dL and/or A1C values of 5.7% to 6.4%. Values lower than these are normal. Numbers higher than these are diagnostic for diabetes.19
Disclaimer: Hope Warshaw was compensated for the development and promotion of this blog from Beneo Institute, the manufacturer of Palatinose™.
References:
1. International Diabetes Federation Diabetes Atlas, 9th ed. Diabetes facts & figures. https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html. Accessed April 17, 2020.
2. Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020. Atlanta, GA: Centers for Disease Control and Prevention, U.S. Dept of Health and Human Services; 2020. Accessed April 17, 2020.
3. Lin, J., Thompson, T.J., Cheng, Y.J. et al. Projection of the future diabetes burden in the United States through 2060. Popul Health Metrics. 2018;16:1-9.
4. JDRF. Type 1 diabetes facts. https://www.jdrf.org/t1d-resources/about/facts/. Accessed April 17, 2020.
5. American Diabetes Association. Economic costs of diabetes in the US in 2017. Diabetes Care. 2018 May;41(5):917–928.
6. Warshaw H. Guest Commentary: Type 2 Diabetes Prevention. Today’s Dietitian. 2018:20(8)31. Link: https://www.todaysdietitian.com/newarchives/0818p31.shtml. Accessed April 17, 2020.
7. Lean MEJ, et al. Durability of a primary care-led weight-management intervention for remission of type 2 diabetes: 2-year results of the DiRECT open-label, cluster-randomised trial. Lancet Diabetes Endocrinol. 2019;7(5):344-355.
8. Look AHEAD Research Group. Eight-year weight losses with an ILI: The Look AHEAD Study. Obesity. 2014;22(1):5-13.
9. Franz MK, Boucher JL, Rutten-Ramos S, et al. Lifestyle weight-loss intervention outcomes in overweight and obese adults with type 2 diabetes. A systematic review and meta-analysis of randomized clinical trials. J Acad Nutr Diet. 2015;115(9):1447-1463.
10. Evert AB, Dennison M, Gardner CD, et al. Nutrition therapy for adults with diabetes or prediabetes: A consensus report. Diabetes Care. 2019;42(5):731-754.
11. Pfeiffer AFH, Keyhani-Nejad F (2018) High glycemic index metabolic damage - a pivotal role of GIP and GLP-1. Trends Endocrinol Metab 29(5):289-299. https://www.cell.com/trends/endocrinologymetabolism/fulltext/S1043-2760(18)30046-8
12. Maresch CC, Pery SF, Theis S, et al. Low glycemic index prototype isomaltulose-update of clinical trials. Nutrients. 2017;9(4): http://www.mdpi.com/2072-6643/9/4/381.
13. Lightowler H, Schweitzer L, Theis S, Henry CJ. Changes in weight and substrate oxidation in overweight adults following isomaltulose intake during a 12-week weight loss intervention: A randomized, double-blind, controlled trial. Nutrients. 2019;11(10):2367.doi: 10.3390/nu11102367.
14. Ang M, Linn T. Comparison of the effects of slowly and rapidly absorbed carbohydrates on postprandial glucose metabolism in type 2 diabetes mellitus patients: a randomized trial. Am J Clin Nutr. 2014;100(4):1059–1068.
15. Brunner S, Holub I, Theis S, et al.Metabolic Effects of Replacing Sucrose by Isomaltulose in Subjects With Type 2 Diabetes: A randomized double-blind trial. Diabetes Care. 2012;35(6):1249–1251.
16. Holub I, Gostner A, Theis S, et al. Novel findings on the metabolic effects of the low glycaemic carbohydrate isomaltulose (Palatinose™). Br J Nutr. 2010;103(12):1730–1737.
17. Keyhani-Nejad F, Kemper M, Schueler R, et al. Effects of Palatinose and Sucrose Intake on Glucose Metabolism and Incretin Secretion in Subjects With Type 2 Diabetes. Diabetes Care. 2016;39(3):e38-e39.
18. Palatinose (isomaltulose). https://www.beneo.com/ingredients/human-nutrition/functional-carbohydrates/palatinose. Accessed April 20, 2020.
19. American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes -2020. Diabetes Care. 43(Supp 1):S14-S31.